Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 40 nº 3 - May / June of 2007
Vol. 40 nº 3 - May / June of 2007
|
ORIGINAL ARTICLE
|
|
Intestinal obstruction after Roux-en-Y gastric bypass by Higa's technique for treatment of morbid obesity: radiological aspects |
|
|
Autho(rs): Ester Moraes Labrunie, Edson Marchiori |
|
|
Keywords: Morbid obesity, Bariatric surgery, Intestinal obstruction, Complication, Radiology, Computed tomography |
|
|
Abstract:
IAssistant Professor of Radiology at Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
INTRODUCTION Obesity is a chronic disease characterized by excessive body fat, whose increase has achieved worldwide epidemic proportions. It is associated with an array of correlated diseases which end up causing early mortality(1,2). Obesity is considered as a morbid condition when the body mass index (BMI) is 40 kg/m² or greater, or 35 kg/m² or greater in patients with some correlated disease (the so called co-morbidity)(2,3). In response to the worldwide epidemic increase of morbid obesity, new treatments have been proposed and improved, with highlights particularly on the development of surgical techniques(4). Nowadays, the surgical technique considered as the most effective for treating morbid obesity is the Roux-en-Y gastric bypass(4). The increase in the frequency of bariatric surgeries demands the radiologist acquaintance with new techniques as well as with functional and anatomical changes resulting from these treatments(5). The postoperative radiological study, the evaluation and early diagnosis of complications pose more and more frequent problems for the radiologist in his/her daily practice. Technical limitations imposed by the biotype and clinical conditions of morbid obese patients may complicate the diagnosis. A detailed and clear-sighted analysis of radiological studies represents a challenge for both the radiologist and the surgical team. Incorrect evaluations or late diagnosis of complications may delay the treatment, and ultimately put the patient's life at risk. Small bowel obstruction occurs in about 1.3%–5% of cases, particularly in patients submitted to videolaparoscopy(4). Laparoscopy results in less surgical trauma, with less formation of adhesions, although with higher incidence of internal hernias(4). On the other hand, the higher incidence of adhesions in laparotomy seems to reduce the propensity to the formation of internal hernias(5). The present study was aimed at discussing radiological findings in ten patients who developed intestinal obstruction as a complication of Roux-en-Y gastric bypass for treatment of morbid obesity.
MATERIALS AND METHODS The present study included ten patients submitted to weight-reducing gastroplasty with Roux-en-Y gastric bypass, presenting with post-operative intestinal obstruction between November/2001 and April/2006. The cases originated from seven different hospital institutions, and the surgeries were performed by five different teams. Four patients were men (40%), and six were women (60%), with ages ranging between 23 and 54 years (mean age, 37.2 years). Nine patients (90%) were submitted to videolaparoscopy surgery, and one (10%) to laparotomy. Fifteen studies were analyzed as follows: nine computed tomographies, two seriographies of esophagus, stomach and jejunum, and four routine studies for acute abdomen. All of the ten patients had surgical confirmation of intestinal obstruction. The radiological findings were compared with the operative report. Indicators as well as possible etiologies of intestinal obstruction were researched. As regards the time period elapsed between surgery and development of intestinal obstruction, the condition was classified into early intestinal obstruction (those occurring up to the seventh post-operative day), and late intestinal obstruction (those occurring after the 30th post-operative day).
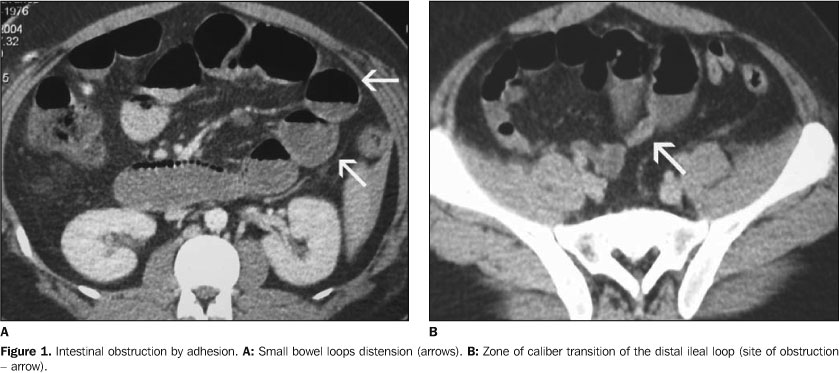
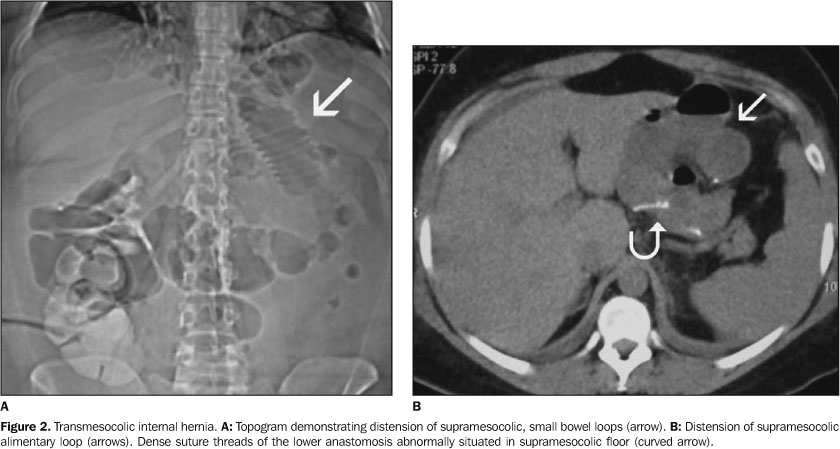
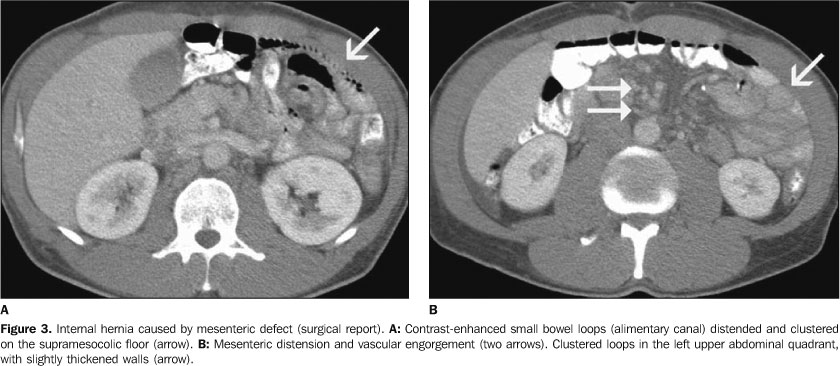
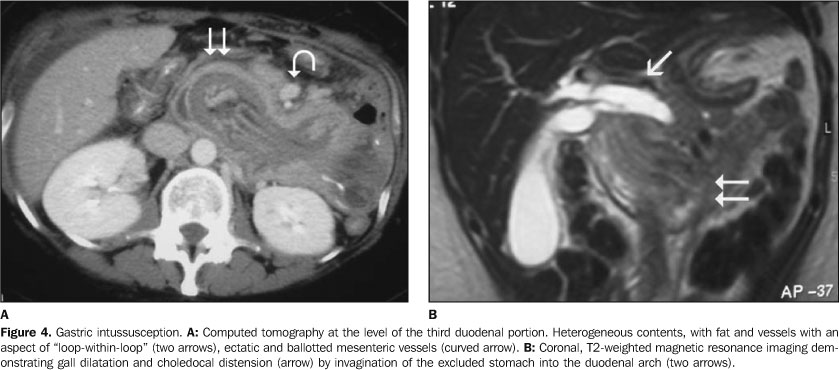
RESULTS Intestinal obstruction occurred in small bowel loop in the ten patients, five of them by internal hernia, three by adhesion, one by umbilical hernia, and one by gastric intussusception. Four patients presented an early obstruction (up to the seventh post operative day), two of them secondary to transmesocolic internal hernia, and two by adhesion in the distal ileum. The other six patients presented late intestinal obstruction (between three months and five years after surgery), three of them related to internal hernias (two transmesocolic and one caused by a mesenteric defect of the lower anastomosis), one caused by umbilical hernia, on by adhesion associated with small bowel volvulus, and one by intussusception of the excluded stomach into the duodenal arch. Surgical reintervention became necessary in all of the patients. In the three cases caused by adhesion, the obstruction occurred in the distal ileal loop (Figure 1). One case occurred in the site of insertion of the laparoscopic trocar, associated with small bowel volvulus. In all of the cases, computed tomography (CT) could identify the zone of caliber transition from the distended loops to the distal, non-distended segment. At surgery, two of these patients presented association with small bowel volvulus in the segment above the obstruction. This finding could be suggested on the CT performed in one of the patients, because of the anterior displacement of the surgical stapling line of the jejuno-jejunal anastomosis. Internal hernias occurred in five patients submitted to videolaparoscopy, four of these hernias being transmesocolic (Figure 2), and one in the mesenteric defect created in the construction of the Roux loop and jejuno-jejunal anastomosis. The four patients with transmesocolic hernia presented distension of the alimentary loop through the transverse mesocolon. One of these patients also presented migration of the lower anastomosis into the supramesocolic space, evidenced by a hyperdense line demonstrating the surgical stapling. The patients with hernia in the mesenteric defect (Figure 3), presented distension of the biliopancreatic loop and excluded stomach. The case of umbilical hernia occurred later in the post-operative period, only in one patient in the group submitted to laparatomy. One case of intussusception of the excluded stomach into the duodenal arch was observed, with secondary displacement of the choledocus. This latest finding could be more clearly observed on a magnetic resonance imaging cholangiography (Figure 4).
DISCUSSION According to Blachar et al.(4), intestinal obstructions occurring between three days and three months in the post-operative period, frequently are secondary to adhesions. Internal hernias, generally, occur later in the post-operative period. Data from our casuistic are different from those reported by these authors. In four of the ten patients studied, obstruction occurred early (up to the seventh post-operative day), and in six, obstruction was late (after the thirtieth post-operative day). Adhesions and internal hernias occurred in both groups. Cases of early transmesocolic internal hernias were observed (five and seven days after in the post-operative period), as well as late adhesions (five years after). So, it seems that the time period elapsed between the bariatric surgery and the onset of symptoms should not be taken into consideration in the etiological evaluation of the intestinal obstruction. Only one (secondary to umbilical hernia) of the ten cases of obstruction occurred in patients submitted primarily to laparotomy. All of the cases of internal hernia and adhesion occurred after videolaparoscopy. This figure, however, is not statistically significant. The literature reports higher incidence of internal hernias in laparoscopies(4) and adhesions in laparotomies(5). According to Blachar et al.(3), the higher incidence of post-laparoscopy internal hernias, compared to laparotomy, would occur because a lower propensity to formation of adhesions as a result of this surgical method. Another predisposition factor may be related to the post-operative reduction in the amount of intraperitoneal fat, with a consequent enlargement of the mesenteric defect(3). A delayed diagnosis, and, consequently, a late surgical reintervention in these patients may lead to gangrene of intestinal segment, resulting in the need of na enterectomy of variable lengths of the small bowel, increasing the complication(6). Two patients were found with intestinal distention in the review of the routine studies for acute abdomen. Initially, these findings were interpreted as adynamic ileum, delaying both the diagnosis and the treatment. Retrospectively, in both cases, the CT performed at that time demonstrated a zone of caliber transition of small bowel loops, characterizing the obstruction. Both patients underwent a quite difficult and complicated post-operative period. Also in both cases, the presence of an anastomosis fistula was observed, possibly secondary to the increased tension on the stapling line, and to the distention above the obstruction, according to the mechanism proposed by Luján et al.(5). Small bowel obstruction may course with non-specific symptoms, such as long-lasting, intermittent abdominal pain, or acute abdominal pain associated with nausea, emesis and constipation(6). Both presentations occurred in our casuistic. A patient who presented with tachycardia as a single clinical post-operative alteration, was submitted to pre-hospital discharge CT, and alterations compatible with early supramesocolic hernia were found. This patient was immediately operated with an excellent recovery. CT has becoming the imaging method of choice for investigation of abdominal symptoms, especially in patients submitted to gastric bypass surgery(6). Patients with non-specific and vague abdominal symptoms should be promptly submitted to oral and intravenous contrast-enhanced CT(7). Besides diagnosing the obstruction, CT allows to advance in the determination of the diagnostic etiology, indicating transmesocolic, mesenteric, umbilical hernias, and gastric intussusception. Also, CT allows the evaluation of intestinal loop distress/thickening and correlated complications, such as pneumoperitoneum, fistulas and collections. Nine of the ten patients with intestinal obstruction were submitted to CT, all of them with abnormal findings. Even in the two cases were a delayed diagnosis was observed, the retrospective review of the images had already indicated the abdominal distension with zone of caliber transition in the small bowel. Blachar et al.(3,8) have discussed tomographic findings of internal hernias, and reported that some findings, if submitted to a clear-sighted analysis, may suggest a diagnosis. The most significant alterations reported by them and also observed in our casuistic, were: small bowel distension suggesting obstruction; clustering of small bowel loops (especially in the left upper abdominal quadrant); engorgement and displacement of mesenteric vessels, absence of omental fat covering the distended/herniated loops and ascites. A finding that we have observed and not reported in this study, in a patient with transmesocolic hernia, was the migration of the anastomosis stapling line towards to the supramesocolic floor of the abdomen visualized as a hyperdense, linear artifact in the intersection between the alimentary and gallbladder loops. Oral contrast-enhanced radiography is also quite sensitive for internal hernias(9). In our casuistic, abdominal plain or contrast-enhanced radiographs of four patients were abnormal, indicating intestinal distension and/or obstruction. The diagnosis of transmesocolic hernia may be suggested by the presence of supramesocolic clustering and distension of small bowel loops. The conventional radiological study may also demonstrate intestinal distension by obstruction of other etiologies (in our casuistic, by adhesion, with or without small bowel volvulus). Intestinal intussusception is a rare complication of this surgery(7,10,11). One case of late intussusception of the excluded stomach into the duodenal arch was observed. The CT finding was highly suggestive of invagination. The secondary complication was the development of jaundice by distention and dilatation of the choledocus, which is best visualized by magnetic resonance imaging. The diagnosis of this complication must be reached as early as possible, considering the reported 10%-mortality in 48 hours, and 50%-mortality after 72 hours(11).
REFERENCES 1. Moura LG Jr, Guimarães SB, Castro-Filho HF, Machado HF, Feijó FC, Vasconcelos PRL. Capella's gastroplasty: metabolites and acute phase proteins changes in midline and bilateral arciform approaches. Arq Gastroenterol 2004;41:215–219. [ ] 2. Blachar A, Federle MP. Gastrointestinal complications of laparoscopic Roux-en-Y gastric bypass surgery in patients who are morbidly obese: findings on radiography and CT. AJR Am J Roentgenol 2002:179:1437–1442. [ ] 3. Blachar A, Federle MP, Pealer KM, Ikramuddin S, Schauer PR. Gastrointestinal complications of laparoscopic Roux-en-Y gastric bypass surgery: clinical and imaging findings. Radiology 2002; 223:625–632. [ ] 4. Blachar A, Federle MP, Pealer KM, Abu Abeid S, Graif M. Radiographic manifestations of normal postoperative anatomy and gastrointestinal complications of bariatric surgery, with emphasis on CT imaging findings. Semin Ultrasound CT MR 2004;25:239–251. [ ] 5. Luján JA, Frutos MD, Hernández Q, et al. Laparoscopic versus open gastric bypass in the treatment of morbid obesity: a randomized prospective study. Ann Surg 2004;239:433–437. [ ] 6. Onopchenko A. Radiological diagnosis of internal hernia after Roux-en-Y gastric bypass. Obes Surg 2005;15:606–611. [ ] 7. Srikanth MS, Keskey T, Fox SR, Oh KH, Fox ER, Fox KM. Computed tomography patterns in small bowel obstruction after open distal gastric bypass. Obes Surg 2004;14:811–822. [ ] 8. Blachar A, Federle MP, Dodson SF. Internal hernia: clinical and imaging findings in 17 patients with emphasis on CT criteria. Radiology 2001; 218:68–74. [ ] 9. Carmody B, DeMaria EJ, Jamal M, et al. Internal hernia after laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis 2005;1:543–548. [ ] 10. Duane TM, Wohlgemuth S, Ruffin K. Intussusception after Roux-en-Y gastric bypass. Am Surg 2000;66:82–84. [ ] 11. Sandrasegaran K, Rajesh A, Lall C, Gomez GA, Lappas JC, Maglinte DD. Gastrointestinal complications of bariatric Roux-en-Y gastric bypass surgery. Eur Radiol 2005;15:254–262. [ ]
Received September 8, 2006.
* Study developed in the Department of Radiology at Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil. |
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554