Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 46 nº 3 - May / June of 2013
Vol. 46 nº 3 - May / June of 2013
|
CASE REPORT
|
|
Heterotaxy syndrome: a case report |
|
|
Autho(rs): Daniel de Souza Carneiro1; Jamil Hussein de Arantes2; Gustavo Veloso de Souza2; Aline Santos Barreto2; Mychaell Luciano Cardoso2; Flávia Gontijo2 |
|
|
Keywords: Heterotaxy syndrome; Situs inversus; Spleen - abnormalities. |
|
|
Abstract: INTRODUCTION
Heterotaxy syndrome (from the Greek heteros different and taxis arrangement) consists of several position and morphology abnormalities of thoracoabdominal organs, which do not fit in the habitual positioning order of organs laterality (situs solitus) or its mirror image (situs inversus)(13). It is a rare entity, and its severity is mainly due to cardiac manifestations. Terms such as asplenia (right atrial isomerism) or polysplenia (left atrial isomerism) are falling into disuse on account of the wide spectrum of anatomical findings, with no pathognomonic characteristic existing which would allow the subclassification under such terms(3). CASE REPORT Female, 28-year-old patient with clinical signs of dyspnea since her childhood, World Health Organization functional class II. At the age of two, the patient was submitted to catheterization, with the following findings: dextrocardia, functionally single atrium, corrected transposition of great vessels, persistence of the arterial canal and interventricular communication. In her adulthood, echocardiogram presented left atrial isomerism and dextrocardia, interruption of the inferior vena cava, atrioventricular septal defect (partial presentation), patent arterial duct with aortopulmonary shunt. Five years ago, significant pulmonary hypertension was diagnosed. Four months ago the patient presented sudden worsening of dyspnea associated with chest pain, mild cyanosis, systolic murmur more audible in the pulmonary focus, with fixed split of S2, physiological vesicular murmurs and oxygen saturation at 70%. A chest computed tomography angiography was requested, and demonstrated dextrocardia and cardiomegaly with predominance of the right chambers, atrial septal defect, increased caliber of the pulmonary trunk (35 mm) with no sign of pulmonary thromboembolism, ectatic ascending aorta with descending segment at the left, infrahepatic vena cava interruption, and azygos vein engorgement from the infradiaphragmatic portion (Figures 1 and 2). Other findings included polysplenia and bilobed lungs, with the main bronchi coursing inferiorly to the pulmonary arteries, and the liver in centrally located, characterizing heterotaxy syndrome (Figures 3 and 4). 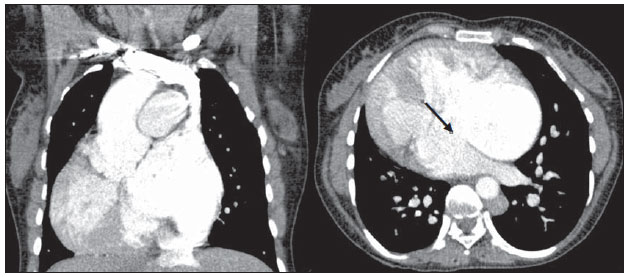 Figure 1. Chest computed tomography angiography demonstrating dextrocardia, cardiomegaly and atrial septal defect (arrow). 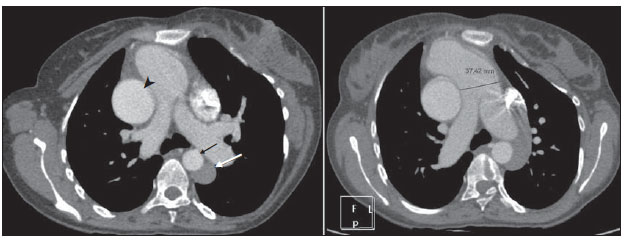 Figure 2. Chest computed tomography angiography showing ectatic ascending aorta, (arrow head) with descending segment at left (small arrow), engorgement of the azygos vein (large arrow), besides increased caliber of the pulmonary artery trunk (figure at right).  Figure 3. Chest computed tomography angiography showing bilobed lungs, with main bronchi coursing inferiorly to the pulmonary artery (arrow). 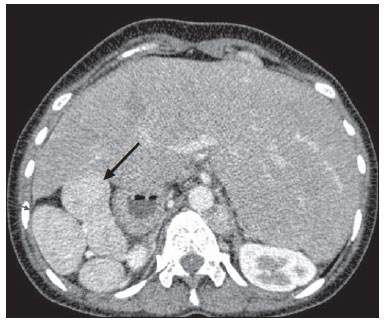 Figure 4. Chest computed tomography angiography demonstrating polysplenia (arrow) and liver centrally located. DISCUSSION The habitual and orderly arrangement of the organs in the human body is determined early in the embryonic development and is based on genetic information(4). The loss of such orderly arrangement may characterize situs inversus or a disordered and variable arrangement (heterotaxy syndrome). Heterotaxy syndrome presents an approximate incidence of 1:10,000 births and is slightly more prevalent in men, at a ratio of 2:1(3,5). Cardiac abnormalities are present in 50% to 100% of patients(3) and, generally, such abnormalities are accountable for the severity and mortality of patients with such a syndrome. Heterotaxy syndrome encompasses a wide range of extracardiac variants, including: urinary system, biliary tract and hepatic abnormalities, duodenal atresia, gastrointestinal malrotation and several cardiovascular alterations(6). The presentation previously called "asplenia" generally presents duplication of structures located in the right side of the body, with trilobed lungs, left atrium with morphology corresponding to the right atrium, centrally positioned liver, left-sided aorta and inferior vena cava, besides intestinal malrotation. In most such cases, death is an early event(3) as a consequence of complications from congenital heart defects, notably the presence of a single atrioventricular chamber. Other reported complications include immunological changes and intestinal volvulus(7). In the presentation previously called "polysplenia" generally there are duplication of the structures in the left side of the body, presenting bilobed lungs, right atrium anatomically identical to the left atrium, liver also centrally positioned, absence of the hepatic segment of the inferior vena cava with continuity through the azygos or hemiazygos vein, besides intestinal malrotation. Cardiac alterations are less frequently found and milder, a fact that explains a higher prevalence of such findings in individuals of more advanced ages(3). The multiplicity and diversity of findings in such a syndrome make the individualization of cases extremely valuable, as most of them do not perfectly fit in any classification Thus, the radiological evaluation is indispensable for the identification and planning of the approach to patients presenting cardiac and immunological complications or surgical conditions, allowing for the evaluation of the alterations present in each patient(8). Acknowledgements The authors wish to thank Dra. Cláudia Juliana Rezende and Dr. Frederico Tadeu Figueiredo Campos, as well as the patient, who promptly agreed to make the images available for the present case report. REFERENCES 1. Kim SJ. Heterotaxy syndrome. Korean Circ J. 2011;41:22732. 2. Kim SJ, Kim WH, Lim HG, et al. Outcome of 200 patients after an extracardiac Fontan procedure. J Thorac Cardiovasc Surg. 2008;136:10816. 3. Applegate KE, Goske MJ, Pierce G, et al. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 1999;19:83752. 4. Shiraishi I, Ichikawa H. Human heterotaxy syndrome from molecular genetics to clinical features, management, and prognosis . Circ J. 2012;76:206675. 5. Lin AE, Ticho BS, Houde K, et al. Heterotaxy: associated conditions and hospital-based prevalence in newborns. Genet Med. 2000;2:15772. 6. Phoon CK, Neill CA. Asplenia syndrome: insight into embryology through an analysis of cardiac and extracardiac anomalies. Am J Cardiol. 1994;73:5817. 7. Mahalik SK, Khanna S, Menon P. Malrotation and volvulus associated with heterotaxy syndrome. J Indian Assoc Pediatr Surg. 2012;17:13840. 8. Vyas HV, Greenberg SB, Krishnamurthy R. MR imaging and CT evaluation of congenital pulmonary vein abnormalities in neonates and infants. Radiographics. 2012;32:8798. 1. Master, MD, Resident of Radiology and Imaging Diagnosis at Hospital Madre Tereza, Belo Horizonte, MG, Brazil. 2. MDs, Residents of Radiology and Imaging Diagnosis at Hospital Madre Tereza, Belo Horizonte, MG, Brazil. * Study developed at Instituto das Pequenas Missionárias de Maria Imaculada Hospital Madre Teresa, Belo Horizonte, MG, Brazil. Mailing Address: Dr. Daniel de Souza Carneiro Centro de Radiologia e Diagnóstico por Imagem Avenida Raja Gabaglia, 1002, Bairro Gutierrez Belo Horizonte, MG, Brazil, 30441-070 E-mail: danielmed124@gmail.com Received October 1st, 2012. Accepted after revision December 3, 2012. |
|
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554