Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 48 nº 5 - Sep. / Oct. of 2015
Vol. 48 nº 5 - Sep. / Oct. of 2015
|
LETTER TO THE EDITOR
|
|
Enteroenteric intussusception in an adult caused by an ileal angiomyolipoma |
|
|
Autho(rs): Rodolfo Mendes Queiroz1; Luana Almeida Botter1; Michela Prestes Gomes2; Rafael Gouvêa Gomes e Oliveira1 |
|
|
Dear Editor,
A white, 32-year-old man was admitted to the emergency department with severe pain principally in the right inferior quadrant of the abdomen, abdominal distension and vomiting for one day. Abdominal radiography, ultrasonography and computed tomography demonstrated small bowel loops distension (Figure 1A) and signs of ileo-ileal invagination associated with intraluminal nodule with fat content compatible with "intussusception head" (Figures 1B, 1C and 1D). Option was made for surgical treatment. 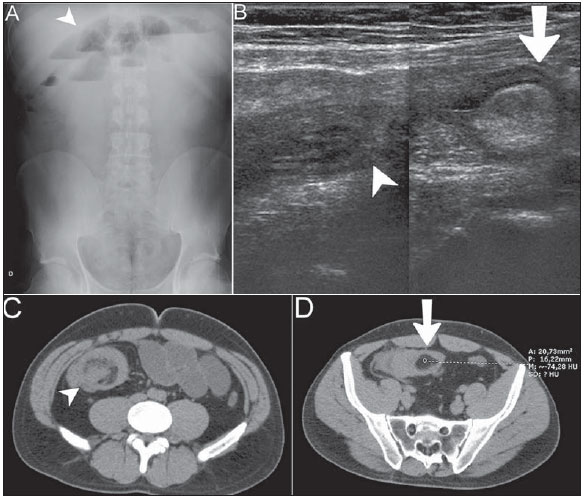 Figure 1. A: Radiographic image demonstrating small bowel loops distension with fluid levels (arrowhead). B: Ultrasonography images composition showing invagination of intestinal wall (arrowhead) adjacent to an echogenic intraluminal nodule (arrow). C,D: Contrastenhanced computed tomography, precontrast phase showing target sign (arrowhead) representing an intussusception adjacent to intraluminal nodule with fat density (arrow). Anatomopathological study in association with immunohistochemical analysis diagnosed angiomyolipoma (AML) as follows: Macroscopy: Bowel loop containing a non-encapsulated delimited, submucosal, polypoid yellowish lesion measuring 3.0 × 2.5 × 2.3 cm, with no sign of malignancy. Microscopy: Masson's trichrome staining diagnosed AML compromising the entire intestinal wall, from the serosa to the mucosa. Immunohistochemical analysis: Desmin, HHF 35, CD31, CD34, protein S100, smooth muscle actin 1 to 4 = positive. Intussusception is the invagination of a proximal intestinal segment with its mesenteric fold with the corresponding vascularization into the lumen of the distal intestinal portion, which may lead to obstruction, inflammatory process and segmental ischemia(1,2). In adult individuals, this condition corresponds to about 5% of the general cases, out of which only 1% of cases cause obstruction(1). In this age group, it is estimated that in 90% of cases one finds organic intraluminal causes called "intussusception heads" (for example, benign neoplasms such as lipoma, or malignant; adenomatous polyps or other polyp types; hamartomas) or extraluminal causes (for example, adhesions, Meckel's diverticulum)(1,3). Intussusception heads in the small bowel are most frequently associated with benign lesions, while in the colon they are most associated with either primary or secondary malignant neoplasias(2). The treatment is generally surgical for organic causes, complications such as obstruction and intestinal ischemia(2,3). The clinical signs of intussusception are related to the occurrence of subocclusion, obstruction and enterorrhagia(3,4). Intussusceptions are classified according the involved intestinal segment, as follows: enteroenteric, colo-colic, ileocolic and ileocecal intussusception(1,3). Typical radiological findings include: "target sign" and "pseudokidney sign"(3). The diagnostic accuracy of ultrasonography approximates to 98%(2), but the method is operator-dependent(5). Computed tomography presents accuracy of 58% to 100%(5). AMLs are benign mesenchymal tumors containing adipose, smooth muscle, epithelial and vascular cells(4,6-8). These tumors and other lesions such as lymphangioleiomyomatosis and clear cell lung tumors were brought together under the classification of PEComas (perivascular epithelioid cell tumors)(4). The prevalence of renal angiomyolipomas ranges from 0.3% to 3%. According to the literature this tumor is sporadic in about 80% of cases, and the remaining cases are associated with lymphangioleiomyomatosis and mainly tuberous sclerosis(6,7). Extrarenal AMLs are extremely rare, and the liver is the most reported site (some other locations include the heart, lungs, retroperitoneum, mediastinum, spinal cord, mucocutaneous, parotid glands, reproductive organs regardless of sex), and its occurrence in the gastrointestinal tract is rarely described(4,6-8) (about 50 cases)(6,7). When located in the gastrointestinal tract their radiological diagnosis is hardly achieved because of their rarity and adipose nature, similarly to lipomas which are much more frequently found(4,7,8). REFERENCES 1. Santos FGPL, Pereira JM, Lima RV, et al. Intussuscepção intestinal secundária a tumor do estroma gastrointestinal (GIST). Rev Imagem. 2007;29:147-51. 2. Rosas GQ, Becker GG. Jejuno e íleo. In: D'Ippolito G, Caldana RP, editors. Gastrointestinal. Série CBR. São Paulo, SP: Elsevier; 2011. p. 173-202. 3. Kim YH, Blake MA, Harisinghani MG, et al. Adult intestinal intussusception: CT appearances and identification of a causative lead point. Radiographics. 2006;26:733-44. 4. Miliaras S, Miliaras D. Angiomyolipoma of the jejunum mimicking metastatic disease in a patient with colonic adenocarcinoma. Surgical Science. 2011;2:52-6. 5. Marinis A, Yiallourou A, Samanides L, et al. Intussusception of the bowel in adults: a review. World J Gastroenterol. 2009;15:407-11. 6. Povo A, Oliveira JMS, Silva R, et al. Angiomiolipoma duodenal. Revista Portuguesa de Cirurgia. 2010;14:107-10. 7. Toye LR, Czarnecki LA. CT of a duodenal angiomyolipoma. AJR Am J Roentgenol. 2002;178:92. 8. Lee CH, Kim JH, Yang DH, et al. Ileal angiomyolipoma manifested by small intestinal intussusception. World J Gastroenterol. 2009;15:1398-400. 1. Documenta - Hospital São Francisco, Ribeirão Preto, SP, Brazil 2. Faculdade de Medicina de Ribeirão Preto da Universidade de São Paulo (FMRP-USP), Ribeirão Preto, SP, Brazil Mailing Address: Dr. Rodolfo Mendes Queiroz Documenta - Centro Avançado de Diagnóstico por Imagem Rua Bernardino de Campos, 980, Centro Ribeirão Preto, SP, Brazil, 14015-130 E-mail: rod_queiroz@hotmail.com |
|
GN1© Copyright 2024 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554