Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 50 nº 5 - Sep. / Oct. of 2017
Vol. 50 nº 5 - Sep. / Oct. of 2017
|
LETTER TO THE EDITOR
|
|
Chordoma of the posterior mediastinum accompanied by synchronous lesion |
|
|
Autho(rs): Bruno Niemeyer de Freitas Ribeiro1; Edson Marchiori2 |
|
|
Dear Editor,
A 53-year-old male patient with a 3-month history of back pain presented with progressive paraparesis, although without loss of sphincter control. Magnetic resonance imaging (MRI) of the dorsal spine (Figures 1A and 1B) showed an expansile lesion with lobulated contours, involving the posterior mediastinum and extending to the vertebral canal, thus reducing the amplitude of the vertebral canal and compressing the medulla. A synchronic lesion of similar appearance, affecting the 12th dorsal vertebra, was observed. The histopathological study revealed large cells with vacuolated cytoplasm and partially vesicular nuclei (some demonstrating prominent nucleoli), with the appearance of physaliferous cells (from the Greek physallis, or bubble), consistent with a diagnosis of chordoma (Figure 1C). 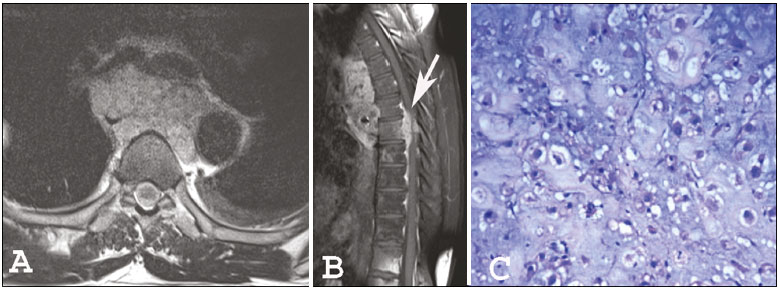 Figure 1. Magnetic resonance imaging scans: axial T2-weighted image (A) and contrast-enhanced sagittal T1-weighted image (B), showing a lesion affecting the posterior mediastinum and invading the vertebral canal (arrow in B). Histopathology (C) revealing physaliferous cells. Recent studies in the radiology literature of Brazil have highlighted the importance of imaging methods in improving the diagnosis of intrathoracic alterations(1-5). Chordomas are slow-growing malignancies derived from primitive remnants of the notochord. They typically occur in the fifth and sixth decades of life(6,7), with a slight predilection for males and preferential involvement of the sacrococcygeal region (50%), followed by the spheno-occipital region (35%), cervical spine, and lumbar spine, occurring only rarely in the dorsal spine and posterior mediastinum(6-8). Symptoms often appear only after the lesion has reached large proportions, with local invasion affecting neurovascular structures. Local recurrence is common when complete resection was not possible. The differential diagnoses of chordoma include metastases, chondrosarcoma, multiple myeloma, neurogenic tumors, among others. Although imaging methods help delineate the lesion, the diagnosis is made on the basis of the histopathological analysis(7). On MRI, most chordomas show isointense or hypointense signals in T1-weighted sequences, whereas they show hyperintense signals in T2-weighted and short-tau inversion-recovery sequences, reflecting their high water content, some lesions containing fibrous septa and therefore showing low signal intensity in T2-weighted sequences(6-8). Gadolinium contrast enhancement tends to be moderate and heterogeneous(6,8). Lesions are often accompanied by bone erosion, which was not observed in the case reported here. Recent studies have highlighted the use of diffusion-weighted imaging in the differentiation between chordomas and chondrosarcomas, reporting that the latter show higher apparent diffusion coefficients(9,10). In addition to an unusual site of involvement, our patient presented the peculiarity of a synchronous lesion. Although some authors have reported similar cases(7,8,11,12), there is no specific criterion for differentiating between a multicentric chordoma and metastatic dissemination. We believe that our case could represent dissemination to the cerebrospinal fluid, because there was involvement of the vertebral canal. The treatment of choice for chordoma is surgical resection with adjuvant radiotherapy, resulting in a disease-free period approximately 2.5 years longer than that achieved after surgical treatment alone(7). Because chordoma is resistant to conventional radiotherapy, other modalities, such as stereotactic radiosurgery, are used. Chordoma does not respond well to chemotherapy, antitumor activity having been observed, in small studies, only with the use of imatinib mesylate(13). Albeit rare, a diagnosis of chordoma should be considered in patients with lesions affecting the posterior mediastinum. In addition, the possibility of synchronous lesions should be investigated in such patients. REFERENCES 1. Guimaraes MD, Hochhegger B, Koenigkam-Santos M, et al. Magnetic resonance imaging of the chest in the evaluation of cancer patients: state of the art. Radiol Bras. 2015;48:33-42. 2. Pessanha LB, Melo AMF, Braga FS, et al. Acute post-tonsillectomy negative pressure pulmonary edema. Radiol Bras. 2015;48:197-8. 3. Barbosa BC, Marchiori E, Zanetti G, et al. Catamenial pneumothorax. Radiol Bras. 2015;48:128-9. 4. Nishiyama KH, Falcão EAA, Kay FU, et al. Acute tracheobronchitis caused by Aspergillus: case report and imaging findings. Radiol Bras. 2014;47:317-9. 5. Fernandes GL, Teixeira AA, Antón AGS, et al. Churg-Strauss syndrome: a case report. Radiol Bras. 2014;47:259-61. 6. Rodallec MH, Feydy A, Larousserie F, et al. Diagnostic imaging of solitary tumors of the spine: what to do and say. Radiographics. 2008;28:1019-41. 7. Aydin AL, Sasani M, Oktenoglu T, et al. A case of chordoma invading multiple neuroaxial bones: report of ten years follow up. Turk Neurosurg. 2013;23:551-6. 8. Lim JJ, Kim SH, Cho KH, et al. Chordomas involving multiple neuraxial bones. J Korean Neurosurg Soc. 2009;45:35-8. 9. Yeom KW, Lober RM, Mobley BC, et al. Diffusion-weighted MRI: distinction of skull base chordoma from chondrosarcoma. AJNR Am J Neuroradiol. 2013;34:1056-61. 10. Freeze BS, Glastonbury CM. Differentiation of skull base chordomas from chondrosarcomas by diffusion-weighted MRI. AJNR Am J Neuroradiol. 2013;34:E113. 11. Badwal S, Pal L, Basu A, et al. Multiple synchronous spinal extra-osseous intradural chordomas: is it a distinct entity? Br J Neurosurg. 2006;20:99-103. 12. Simon SL, Inneh IA, Mok CL, et al. Multiple epidural lumbar chordomas without bone involvement in a 17-year-old female: a case report. Spine J. 2011;11:e7-10. 13. Casali PG, Stacchiotti S, Sangalli C, et al. Chordoma. Curr Opin Oncol. 2007;19:367-70. 1. Instituto Estadual do Cérebro Paulo Niemeyer, Rio de Janeiro RJ, Brazil 2. Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil Mailing address: Dr. Bruno Niemeyer de Freitas Ribeiro Instituto Estadual do Cérebro Paulo Niemeyer Departamento de Radiologia Rua do Rezende, 156, Centro Rio de Janeiro, RJ, Brazil, 20231-092 E-mail: bruno.niemeyer@hotmail.com |
|
GN1© Copyright 2024 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554