Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 53 nº 6 - Nov. / Dec. of 2020
Vol. 53 nº 6 - Nov. / Dec. of 2020
|
ADVANCES IN RADIOLOGY
|
|
Computed tomography-guided biopsy of breast lesions: a viable option for selected cases |
|
|
Autho(rs): Vinicius Cardona Felipea; Luciana Grazianob; Paula Nicole Vieira Pinto Barbosac; Almir Galvão Vieira Bitencourtd |
|
|
INTRODUCTION
The imaging methods of choice to guide percutaneous biopsies of suspected breast lesions are mammography, ultrasound, and magnetic resonance imaging (MRI) (1). However, in some cases it may be difficult to perform a biopsy due to the characteristics of the lesion and its location. This occurs mainly in lesions identified only at MRI since biopsy guided by this method is still an expensive procedure with limited availability in Brazil(2). Computed tomography (CT)-guided percutaneous biopsy is a well-established technique for diagnosing lesions in different parts of the body(3). Although few reports in the literature address the use of this technique for performing breast lesion biopsies, CT guidance is possible as long as the lesion is well characterized by this method. Despite the additional radiation dose, this procedure is faster and less expensive than MRI-guided biopsy(4,5). This study aimed to present the technique of CT-guided breast biopsy, which can be useful in selected cases when it is not possible or technically feasible to guide the biopsy by conventional methods. PROCEDURE We describe two cases where a CT-guided large-core needle biopsy of breast lesions was performed. The procedures were performed jointly by medical radiologists who are specialized in breast imaging and interventional radiology. The procedures were indicated after identifying the lesion in previous CT examinations and in response to the difficulty in performing biopsy by other methods. After consenting to the procedure, patients were placed in a supine or oblique position on the CT table with their arms raised, using silicone cushions to adjust their position. Asepsis and local anesthesia were performed, followed by the introduction of a semi-automatic cutting needle, removal of four to six fragments for histological analysis, and placement of a metal clip. Sequential tomographic acquisitions were used to evaluate the progression and final positioning of the needle. No complications were observed. In the first case, a 50-year-old patient showed a focal asymmetry in the posterior depth of the inner quadrants of the left breast on mammography, which was not characterized on ultrasound (Figure 1). A stereotactic-guided biopsy was attempted, but access was not possible due to the lesion location. A previous chest CT scan of the patient showed a enhancement mass in the same topography of the mammographic finding. A CT-guided biopsy was performed, and the histological result was invasive tubular carcinoma.  Figure 1. A: Mammography showing focal asymmetry in the posterior depth of the inner quadrants of the left breast (circle). B: CT showing a enhancing mass at the same topography of the mammographic finding (circle) and needle positioned to perform the biopsy. In the second case, a 39-year-old patient with cancer in the left breast underwent pretreatment MRI, which showed a new lesion in the right breast, not characterized by ultrasound and mammography (Figure 2). The patient had undergone a chest and abdomen CT scan for systemic staging, which showed the enhancing lesion in the right breast. Thus, a CT-guided procedure was performed. The histological result showed invasive ductal carcinoma. 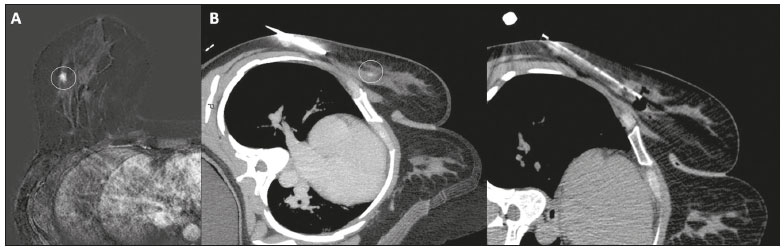 Figure 2. A: MRI showing a mass with irregular margins in the outer quadrants of the right breast (circle). B: CT showing the same mass in the right breast (circle) and needle positioned to perform the biopsy. CONCLUSION CT-guided large-core needle biopsy proved to be a safe and effective method for sampling breast lesions in selected cases where it is not possible to perform the procedure by conventional methods. REFERENCES 1. OFlynn EA, Wilson ARM, Michell MJ. Image-guided breast biopsy: state-of-the-art. Clin Radiol. 2010;65:25970. 2. Chevrier MC, David J, El Khoury M, et al. Breast biopsies under magnetic resonance imaging guidance: challenges of an essential but imperfect technique. Curr Probl Diagn Radiol. 2016;45:193204. 3. Gupta S, Madoff DC. Image-guided percutaneous needle biopsy in cancer diagnosis and staging. Tech Vasc Interv Radiol. 2007;10:88101. 4. Mendel JB, Long M, Slanetz PJ. CT-guided core needle biopsy of breast lesions visible only on MRI. AJR Am J Roentgenol. 2007;189: 1524. 5. Graziano L, Barbosa PNVP, Travesso DJ, et al. CT-guided biopsy of breast lesions: when should it be considered? Breast J. 2019;25: 10502. 1. Imaging Department, A.C.Camargo Cancer Center, São Paulo, SP, Brazil a. https://orcid.org/0000-0001-5727-5070 b. https://orcid.org/0000-0001-6953-4869 c. https://orcid.org/0000-0002-3231-5328 d. https://orcid.org/0000-0003-0192-9885 Correspondence: Dr. Almir Galvão Vieira Bitencourt A.C.Camargo Cancer Center Departamento de Imagem Rua Professor Antônio Prudente, 211, Liberdade São Paulo, SP, Brazil, 01509-010 Email: almir.bitencourt@accamargo.org.br Received 25 September 2019 Accepted after revision 1 December 2019 |
|
GN1© Copyright 2024 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554