Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 54 nº 3 - May / June of 2021
Vol. 54 nº 3 - May / June of 2021
|
LETTERS TO THE EDITOR
|
|
Portal vein embolization, biembolization, and liver venous deprivation |
|
|
Autho(rs): José Hugo Mendes Luza; Tiago Bilhimb |
|
|
Dear editor
We read with great interest the article Liver venous deprivation prior to hepatectomy: an interventional radiology procedure, authored by Alves et al.(1), in a recent issue of Radiologia Brasileira. This is an excellent addition to the Advances in Radiology section of the journal, which highlights the latest developments in medical practice in Brazil. Liver regeneration prior to major hepatectomy is decisive in cancer management because it allows these potentially curative surgical procedures to be performed in otherwise inoperable patients, thus improving survival outcomes(2). Portal vein embolization (PVE), used for decades as a method of inducing liver hypertrophy(3), has recently been used in combination with embolization of one or more hepatic veins(4). Alves et al.(1) described concomitant PVE and proximal right hepatic vein embolization with a vascular plug. This technique might be more appropriately designated biembolization(5), being slightly different from liver venous deprivation (LVD). The LVD procedure has been described as: PVE plus proximal and distal embolization of the hepatic veins. Proximal embolization of the hepatic vein is accomplished with a vascular plug, as in biembolization, whereas distal embolization of the hepatic vein is achieved with N-butyl-cyanoacrylate (NBCA) plus lipiodol, as in LVD(2). Why might this be relevant? Invariably, venovenous collaterals between liver segments V/VIII and IV are present(6) and will increase in size after plug deployment(4). Distal embolization with a liquid embolic agent (i.e., NBCA) not only eliminates flow in the target vein but also occludes those collaterals, which might have benefits in terms of liver hypertrophy induction. In addition, biembolization and LVD may require different technical approaches: LVD is usually performed through a percutaneous trans-hepatic approach(4,7), making it easier to inject liquid embolic agents after plug deployment, whereas biembolization is performed through a transjugular approach (Figure 1). 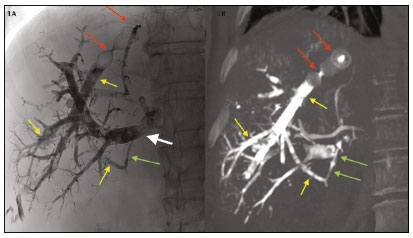 Figure 1. Fluoroscopic image (1A) obtained immediately after LVD and contrastenhanced coronal CT (1B) obtained 14 days after LVD. Note the vascular plug (red arrows) placed in the right hepatic vein for proximal embolization and NBCA plus lipiodol occluding the distal branches (yellow arrows). Note also NBCA plus lipiodol occluding a venovenous collateral (green arrows) and right portal vein embolization with NBCA plus lipiodol (white arrow). Segment IV PVE, which was performed by Alves et al.(1), has been reported to induce additional liver hypertrophy(8). However, segment IV embolization is controversial: the segment IV portal branches are usually numerous and tiny, which increases the procedure time and the degree of technical difficulty; liquid embolic agents are trickier to use, because any reflux would cause nontarget embolization of liver segments II and III; due to the degree of technical difficulty, suboptimal embolization of segment IV might be an issue(9); and segment IV is the main territory for systemic-portal venous shunts, possibly decreasing the efficacy of the procedure(10). To overcome the limitations of PVE of segment IV, a more aggressive form of LVD has been proposedextended LVD(11)which consists of LVD plus middle hepatic vein embolization. Extended LVD has been shown to be safe and highly effective, promoting an unparalleled 53.4% increase in liver volume within only seven days(11). Future studies focusing on patient selection are needed. When and how to choose from such a variety of interventional tools? How to best predict post-hepatectomy liver failure? How can we choose between volumetric computed tomography and liver function studies (e.g., 99mTc-mebrofenin hepatobiliary scintigraphy, gadoxetic acid-enhanced magnetic resonance imaging, and indocyanine green retention test)or should we perform both? Most importantly, when is the liver ready for major surgery? How can we safely accelerate this preoperative process? Answering such questions are the reason for having multidisciplinary team meetings that allow personalized medical care, with input from different medical perspectives. We want to congratulate the authors not only for obtaining a regenerative outcome that allowed successful major hepatectomy within 41 days after embolization but also for highlighting the potential role and advantages of LVD versus PVE, providing grounds to expand future studies in this field(12). REFERENCES 1. Alves VPV, Azevedo A, Araujo DA, et al. Liver venous deprivation prior to hepatectomy: an interventional radiology procedure. Radiol Bras. 2021;54:623. 2. Giglio MC, Giakoustidis A, Draz A, et al. Oncological outcomes of major liver resection following portal vein embolization: a systematic review and meta-analysis. Ann Surg Oncol. 2016;23:370917. 3. Luz JHM, Gomes FV, Coimbra E, et al. Preoperative portal vein embolization in hepatic surgery: a review about the embolic materials and their effects on liver regeneration and outcome. Radiol Res Pract. 2020;2020:9295852. 4. Guiu B, Chevallier P, Denys A, et al. Simultaneous trans-hepatic portal and hepatic vein embolization before major hepatectomy: the liver venous deprivation technique. Eur Radiol. 2016;26:425967. 5. Le Roy B, Perrey A, Fontarensky M, et al. Combined preoperative portal and hepatic vein embolization (biembolization) to improve liver regeneration before major liver resection: a preliminary report. World J Surg. 2017;41:184856. 6. Gai YH, Cai SF, Guo WB, et al. Sonographic classification of draining pathways of obstructed hepatic veins in Budd-Chiari syndrome. J Clin Ultrasound. 2014;42:13442. 7. Panaro F, Giannone F, Riviere B, et al. Perioperative impact of liver venous deprivation compared with portal venous embolization in patients undergoing right hepatectomy: preliminary results from the pioneer center. Hepatobiliary Surg Nutr. 2019;8:32937. 8. Kishi I, Madoff DC, Abdalla EK, et al. Is embolization of segment 4 portal veins before extended right hepatectomy justified? Surgery. 2008;144:74451. 9. de Baere T, Teriitehau C, Deschamps F, et al. Predictive factors for hypertrophy of the future remnant liver after selective portal vein embolization. Ann Surg Oncol. 2010;17:20819. 10. Breen DJ, Rutherford EE, Stedman B, et al. Intrahepatic arterioportal shunting and anomalous venous drainage: understanding the CT features in the liver. Eur Radiol. 2004;14:224960. 11. Guiu B, Quenet F, Escal L, et al. Extended liver venous deprivation before major hepatectomy induces marked and very rapid increase in future liver remnant function. Eur Radiol. 2017;27:334352. 12. Luz JHM, Gomes FG, Costa NV, et al. BestFRL trial: liver regeneration at CT before major hepatectomies for liver cancera randomized controlled trial comparing portal vein embolization with N-butyl-cyanoacrilate plus iodized oil versus polyvinyl alcohol particles plus coils. Radiology. 2021 April 6;204055. Online ahead of print. Department of Interventional Radiology, Curry Cabral Hospital, and NOVA Medical School, Universidade NOVA de Lisboa, Lisbon, Portugal. a. https://orcid.org/0000-0002-1222-850X b. https://orcid.org/0000-0003-3044-8474 Correspondence: José Hugo Mendes Luz, MD Hospital Curry Cabral Serviço de Radiologia de Intervenção Rua da Beneficência 8, 1069-166 Lisboa, Portugal Email: jhugoluz@gmail.com / josehugo@rivoa.com.br |
|
GN1© Copyright 2024 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554