Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 41 nº 2 - Mar. / Apr. of 2008
Vol. 41 nº 2 - Mar. / Apr. of 2008
|
CASE REPORT
|
|
Kaposi sarcoma related to acquired immunodeficiency syndrome: hepatic findings on computed tomography and magnetic resonance imaging |
|
|
Autho(rs): Daniel Nobrega da Costa, Publio Cesar Cavalcante Viana, Rosângela Pereira Maciel, Eloisa Maria Mello Santiago Gebrim, Manoel de Souza Rocha |
|
|
Keywords: Kaposi sarcoma, Acquired immunodeficiency syndrome, Liver disease, Cancer, Computed tomography, Magnetic resonance imaging |
|
|
Abstract:
IMDs, Residents in Radiology and Imaging Diagnosis at Instituto de Radiologia do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (InRad/HC-FMUSP), São Paulo, SP, Brazil
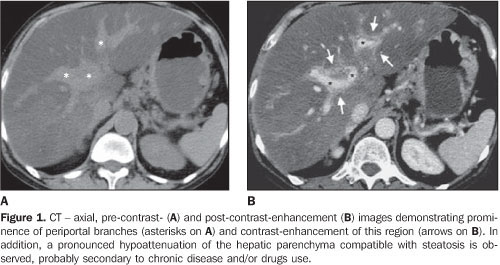
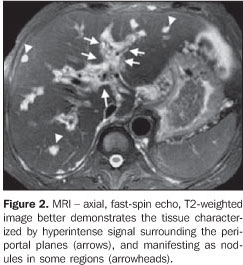
CASE REPORT A 47-year-old male patient previously diagnosed with acquired immunodeficiency syndrome (AIDS) has sought hospital assistance because of recurrent and progressive episodes of melena in the two previous months. Clinical examination has demonstrated nodules and disseminated violaceous plaques on the skin, predominantly in the lower limbs. Based on this clinical context, the diagnosis of AIDS-related Kaposi sarcoma (KS) has been suggested and later confirmed by skin biopsy. The patient underwent upper digestive endoscopy and colonoscopy to investigate the melena, and gastroesophageal involvement was detected. Additionally, chest/abdominal computed tomography (CT) and magnetic resonance imaging (MRI) have been requested to rule out visceral involvement. Chest CT has demonstrated pronounced hepatic steatosis and prominence of periportal spaces (Figure 1A), with exuberant periportal contrast-enhancement (Figure 1B). Abdominal MRI has clearly demonstrated the presence of tissue surrounding the portal branches (arrows on the Figure 2) and the overall nodular involvement of the hepatic parenchyma.
DISCUSSION KS is a low-grade mesenchymal neoplasm initially described by Moritz Kaposi in 1872. Generally, this disease affects blood and lymphatic vessels, most frequently on the skin, although frequently may be found in other organs. Presently four variants of the disease are found with different clinical presentations: 1) classic (sporadic or Mediterranean) KS; 2) endemic (African) KS; 3) iatrogenic (organ transplant-related) KS; 4) AIDS-related KS. For decades before the AIDS breakout and the increase in the number of organ transplants, KS used to be viewed as a very rare disease. Although its etiology is still to be fully understood, the AIDS- and transplant-related forms of the disease are clearly associated with immunosuppression or immunodeficiency. Infection by the human herpes virus 8 – HHV8 and other factors have been implied in the development of the disease. The HHV8 transmission mechanism also is still to be understood, but epidemiological studies indicate the male-to-male sexual contact as an important transmission route to be considered(1). Generally, the disease affects individuals with low CD4 lymphocytes counts (< 150–200 cell/mm³). Most frequent sites of visceral involvement in AIDS-related KS are lymphonodi (72% of cases), lungs (51%), gastrointestinal tract (48%), liver (34%), and spleen (27%)(2). AIDS-related KS is the most frequent hepatic neoplasm in AIDS patients. Cutaneous involvement is present in the majority of cases and represents a useful information in the diagnostic approach in cases where other hepatic conditions must be taken into consideration in the differential diagnosis. It is important to note that, in these cases, no specific treatment is required, and the condition alone does not affect the clinical progression of the patients(1). Macroscopically, multiple brown-violaceous, spongiform nodules are observed, diffusely scattered over the periportal conjunctive tissue(2). Ultrasonography demonstrates multiple hyperechogenic bands and nodules adjacent to the portal branches, besides the heterogeneous texture of the hepatic parenchyma(2,3). CT demonstrates multiple, small nodules diffusely distributed throughout the liver or predominantly found adjacent to the periportal branches, prominence and contrast-enhancement of periportal and hilar planes secondary to the presence of neoplastic tissue(3,4). In cases of predominantly nodular hepatic presentation of KS, metastatic disease, fungal microabscesses and multiple hemangiomas should be taken into consideration as differential diagnoses(3,4). The exuberant periportal hepatic contrast-enhancement identified at CT and MRI also can be found in schistosomal patients with periportal metastatic infiltration and in cases of diffuse, infiltrating cholangiocarcinoma(4). Although the hepatic involvement resulting from AIDS-related KS is rarely diagnosed or symptomatic, infrequently contributing to the morbimortality in these patients, it is important to recognize and differentiate this condition from other hepatic diseases. Considering that percutaneous biopsies may result in massive hemorrhage and hemoperitoneum, the radiologist must be familiarized with the diagnosis to assist in avoiding this complication.
REFERENCES 1.Tappero JW, Conant MA, Wolfe SF, et al. Kaposi's sarcoma. Epidemiology, pathogenesis, histology, clinical spectrum, staging criteria and therapy. J Am Acad Dermatol. 1993;28:371–95. [ ] 2.Restrepo CS, Martinez S, Lemos JA, et al. Imaging manifestations of Kaposi sarcoma. Radiographics. 2006;26:1169–85. [ ] 3.Luburich P, Bru C, Ayuso MC, et al. Hepatic Kaposi sarcoma in AIDS: US and CT findings. Radiology. 1990;175:172–4. [ ] 4.Hammerman AM, Kotner LM Jr, Doyle TB. Periportal contrast enhancement on CT scans of the liver. AJR Am J Roentgenol. 1991;156:313–5. [ ] Received November 22, 2006. Accepted after revision January 31, 2007. * Study developed at Instituto de Radiologia do Hospital das Clínicas da Faculdade de Medicina da Universidade de São Paulo (InRad/HC-FMUSP), São Paulo, SP, Brazil. |
|

Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554