Radiologia Brasileira - Publicação Científica Oficial do Colégio Brasileiro de Radiologia
AMB - Associação Médica Brasileira CNA - Comissão Nacional de Acreditação
 Vol. 49 nº 4 - July / Aug. of 2016
Vol. 49 nº 4 - July / Aug. of 2016
|
LETTER TO THE EDITOR
|
|
Aortic arch anomaly in an adult patient: a case of right aortic arch with aberrant left subclavian artery and Kommerell's diverticulum |
|
|
Autho(rs): Alexandre Ferreira Silva1; José Antônio dos Santos2 |
|
|
Dear Editor,
We report the case of a 54-year-old male presenting with vague symptoms of discomfort when swallowing. The patient underwent magnetic resonance imaging of the chest. The examination showed right aortic arch with an aberrant left subclavian artery and Kommerell's diverticulum (Figures 1 and 2). 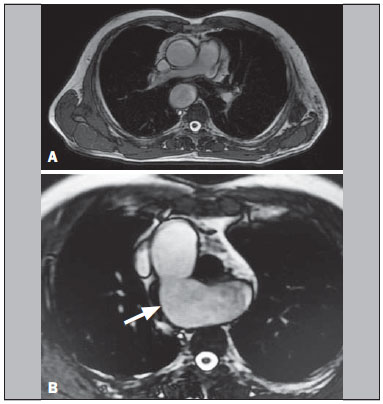 Figure 1. A,B: Axial T2-weighted spin-echo magnetic resonance imaging showing right aortic arch (arrow).  Figure 2. Coronal T2-weighted spin-echo magnetic resonance imaging showing Kommerell's diverticulum (arrow). Thoracic diseases of vascular origin have been the subject of a number of recent publications in the radiology literature of Brazil(15). First described by Fioratti et al., right aortic arch is an uncommon birth defect, of unknown cause, occurring in 0.05% of the general population. It is often asymptomatic but can be accompanied by dysphagia and complications arising from the formation of an aneurysm. Such an aneurysm generally occurs at the origin of the left subclavian artery and is known as Kommerell's aneurysm or Kommerell's diverticulum, which can cause compression of mediastinal structures or can rupture spontaneously(6-13). In children, the symptoms can also be associated with existing congenital cardiac abnormalities(7). Various systems for classifying right aortic arch have been proposed. The most widely used classification system is that devised by Edwards, who described three main types of right aortic arch: type I, with mirror-image branching of the major arteries; type II, with an aberrant subclavian artery; and type III, with an isolated subclavian artery (connected to the pulmonary artery via the ductus arteriosus)(8). In the case presented here, the variant was classified as an Edwards type II right aortic arch, which accounts for approximately 40% of all cases(7). In an autopsy study cited by Faucz et al.(7), 50% of cases of right aortic arch were associated with an aberrant left subclavian artery, which can be located behind the esophagus (in 80%), between the trachea and the esophagus (in 15%), or anterior to the trachea (in 5%). In some cases, right aortic arch is associated with a congenital heart defect(7,9,10). The treatment of right aortic arch is generally surgical and is quite complex. Preoperative imaging tests are extremely important for the surgical planning, which relies heavily on knowledge of the anatomical distribution of the local structures, as well as of the size and extent of the aneurysm. Although outpatient treatment is an option, endovascular repair has been performed successfully(7,11). The indication for surgical intervention in right aortic arch continues to be a subject of debate. Surgical intervention is considered an acceptable option when the diameter of the orifice of the diverticulum is > 30 mm or the diameter of the descending aorta adjacent to the diverticulum is > 50 mm(11). REFERENCES 1. Neves PO, Andrade J, Monção H. Coronary anomalies: what the radiologist should know. Radiol Bras. 2015;48:23341. 2. Herrero Lara JA, de Araújo Martins-Romêo D, Caparrós Escudero C, et al. Hybrid treatment of penetrating aortic ulcer. Radiol Bras. 2015;48:1924. 3. Batista MN, Barreto MM, Cavaguti RF, et al. Pulmonary artery sarcoma mimicking chronic pulmonary thromboembolism [Letter]. Radiol Bras. 2015;48:3334. 4. Amaral RH, Souza VVS, Nin CS, et al. Aortic lesion simulating pulmonary disease: a case report. Radiol Bras. 2014;47:3202. 5. Araújo Neto CA, Andrade ACO, Badaró R. Intima-media complex in the investigation of atherosclerosis in HIV-infected patients [Letter]. Radiol Bras. 2014;47(1):x. 6. Sprong DH, Cutler NL. A case of human right aorta. Anat Rec. 1930;45:36575. 7. Faucz RA, Furlan S, Barros AS, et al. Arco aórtico direito com artéria subclávia esquerda aberrante e divertículo de Kommerell. Radiol Bras. 2005;38:3814. 8. Edwards JE. Anomalies of the derivatives of the aortic arch system. Med Clin North Am. 1948;32:92549. 9. Costa RN, Andrade IS, Reyes RO, et al. Arco aórtico direito com divertículo de Kommerell. Rev Bras Cardiol Invas. 2009;17:27980. 10. Kimura-Hayama ET, Meléndez G, Mendizábal AL, et al. Uncommon congenital and acquired aortic diseases: role of multidetector CT angiography. Radiographics. 2010;30:7998. 11. Tanaka A, Milner R, Ota T. Kommerell's diverticulum in the current era: a comprehensive review. Gen Thorac Cardiovasc Surg. 2015;63:24559. 12. Barranhas AD, Indiani JM, Marchiori E, et al. Atypical presentation of Kommerells diverticulum. Arq Bras Cardiol. 2009;93:e8890, e1013. 13. Barranhas AD, Santos AASMD, Coelho-Filho OR, et al. Cardiac magnetic resonance imaging in clinical practice. Radiol Bras. 2014;47:18. 1. Ecotomo S/C Ltda., Belém, PA, Brazil 2. Dimagem Diagnóstico por Imagem, Belém, PA, Brazil Mailing address: Dr. Alexandre Ferreira Silva Rua Bernal do Couto, 93/1202, Umarizal Belém, PA, Brazil, 06055-080 E-mail: alexandreecotomo@oi.com.br |
|
GN1© Copyright 2024 - All rights reserved to Colégio Brasileiro de Radiologia e Diagnóstico por Imagem
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554
Av. Paulista, 37 - 7° andar - Conj. 71 - CEP 01311-902 - São Paulo - SP - Brazil - Phone: (11) 3372-4544 - Fax: (11) 3372-4554